Breastfeeding is key to child survival, particularly in low- and middle-income countries, and important for optimal child growth and development worldwide. Starting breastfeeding within one hour of birth (known as ‘early initiation of breastfeeding’, or EIBF) offers the infant and mother the best chance for success with breastfeeding, and makes it more likely that the infant will be exclusively breastfed (no other liquid or food) for the recommended first six months.
Both EIBF and exclusive breastfeeding for the first six months reduce infant deaths. Breastmilk has all the nutrients and calories babies need, and the very first milk, colostrum, has essential antibodies and other immune factors that help the newborn’s intestinal development and prevent infections (Victora et al., 2016). Starting late, even if within the first day but not in the first hour, can endanger the life of an infant. If breastfeeding is withheld for more than a day then that risk doubles (Smith et al., 2017). When mothers do not initiate
breastfeeding early, chances are poor that the infant will breastfeed exclusively for the recommended six months, or breastfeed at all (Morse et al., 1990).
Unfortunately, less than half of infants (42%) worldwide start breastfeeding within one hour of birth (Unicef and World Health Organization, 2018). The reasons for this are cultural and social, such as harmful norms that encourage mothers to discard colostrum and use other foods in the first day or days, such as honey, sugar-water, cow’s milk, or herbal pastes (Sundaram et al., 2016). Also, hospitals and health facilities often do not support EIBF, which requires early and frequent skin to skin contact and keeping the mother and infant together. Facilities may follow outdated practices of giving sugar-water to newborns, and/or provide breastmilk substitutes (BMS), despite the International Code of Marketing of BMS which prohibits this practice.
EIBF is (or should be) a practice that is relatively easy to implement because it does not have to be sustained day after day as is the case with exclusive breastfeeding for six months. A mother either does it as soon as the baby is born, or not. Also, women do not usually give birth alone, no matter where they are. Giving birth in a health facility, the norm for many countries today, provides the assurance that the mother is likely to have a skilled birth attendant with her. These skilled birth attendants, since they work within an institution, are easy to reach with guidance, coaching and supportive policies.
Scaling an EIBF approach in Vietnam
Alive & Thrive (A&T), is a global nutrition initiative that has been working to improve breastfeeding (and other maternal, infant, and young child) practices since 2009.1 From 2009 to 2014, the initiative demonstrated that it was possible to improve breastfeeding at scale in three different contexts: Ethiopia, Bangladesh and Vietnam (see Figure 1). Guided by its now-proven framework for implementing infant and young child feeding at scale (see Figure 2), A&T reached millions of mothers with children under 2 years of age through a combination of policy advocacy, interpersonal and mass communication, and community mobilisation on infant and young child feeding. Systematic measurement, learning, and evaluation were also essential; data drove advocacy, and motivated decision makers.

Figure 1: Rapid, large-scale improvements in breastfeeding are possible
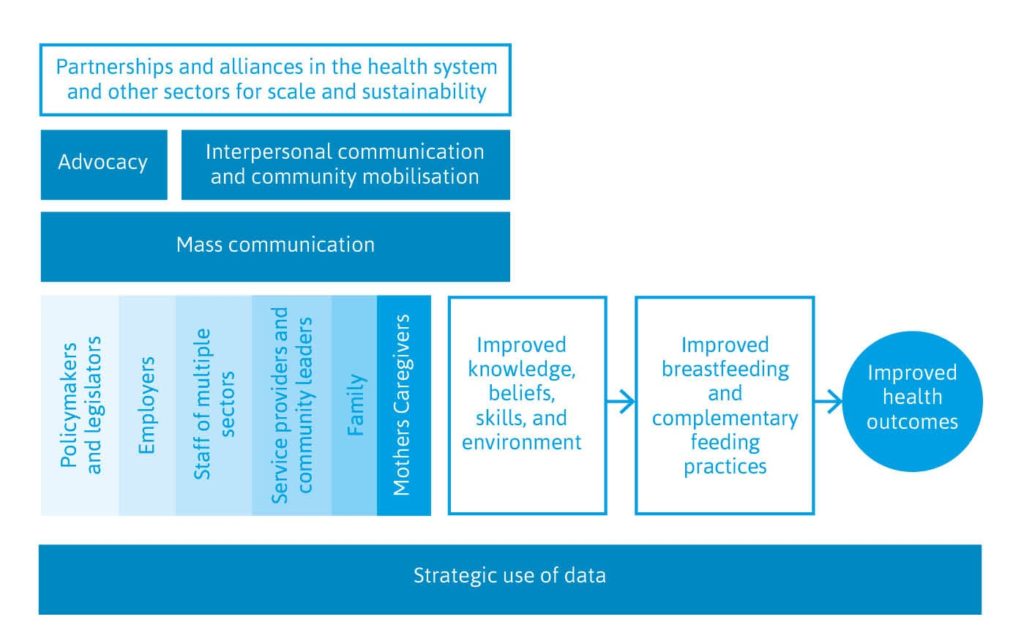
Figure 2: Framework for implementing infant and young child feeding at scale
In Vietnam, following the initial success, A&T began to improve on and scale-up its approach throughout the region. At that time, however, A&T realised that the improvements made in breastfeeding did not include EIBF. While exclusive breastfeeding to six months increased from 19% to 58% (Menon et al., 2016), EIBF was declining (see Figure 3). Almost all births in Vietnam occurred in a health facility; however, it was common practice to separate the baby from the mother at birth before breastfeeding was initiated. A&T had worked with the government’s Ministry of Health on measures to help mothers and caregivers understand and be successful in providing breastmilk exclusively for six months, but it had not addressed what was happening at birth to support breastfeeding.
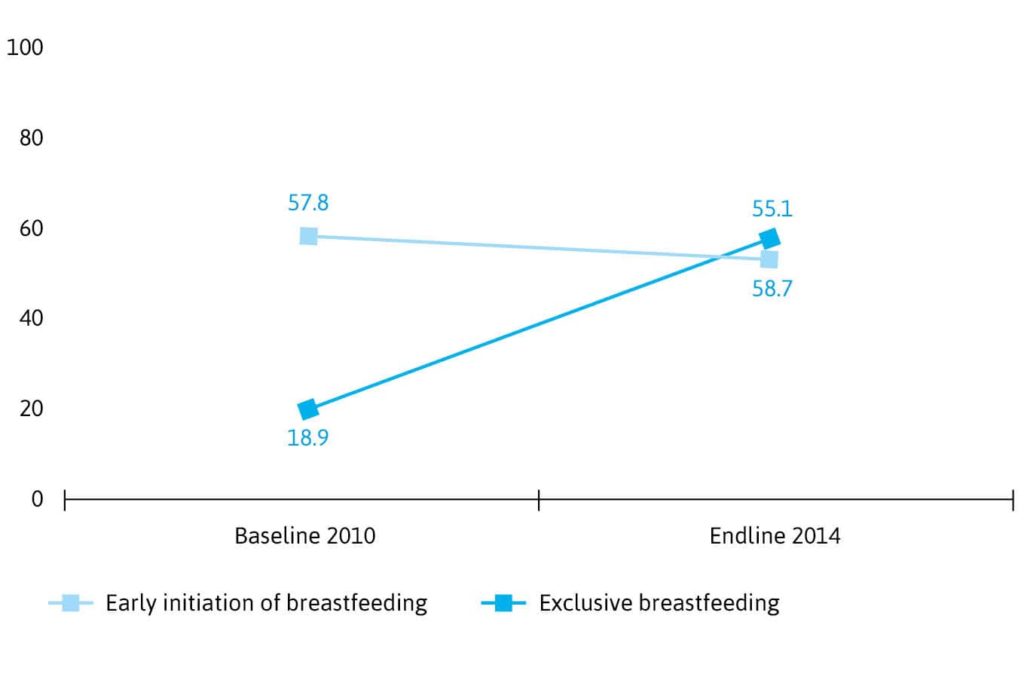
Figure 3: Percentage change in breastfeeding practices in A&T interventions and non-intervention areas
A&T and the Ministry of Health began to address this challenge in 2014. At about the same time, the World Health Organization (WHO) and Unicef also realised the need to confront low rates of EIBF. They finalised the Action Plan for Healthy Newborn Infants in the Western Pacific Region, which established a set of early essential newborn care (EENC) practices to occur at every birth, including immediate skin-to-skin contact and EIBF. The Ministry of Health and partners turned this regional action plan into specific EENC guidelines for Vietnam. Together they tackled early initiation of breastfeeding using the same effective approaches that had improved the rates of exclusive breastfeeding, with a focus on provider behaviours, institutional guidelines, and outreach to the community.
A&T directly supported about 800 health staff and 100 hospitals in seven provinces to begin implementation of the EENC guidelines. National trainers received training and local champions of breastfeeding were identified to train facility staff in the new guidelines. Coaching and supportive supervision mechanisms were put in place, and data were collected to track the outcomes. The result was that EIBF for vaginal deliveries reached 90% or higher in the A&T- supported facilities.
But data showed a significant difference between EIBF after vaginal deliveries and after Caesarian-section deliveries: only 30% of mothers were able to practice EIBF after a C-section. Monitoring data revealed that providers lacked the skills to follow EENC guidelines after a C-section, and did not have sufficient personnel to give these mothers the extra support they need. Sharing the data convinced the Ministry of Health to create national guidelines for EENC that were specific to C-section deliveries. In late 2016, using its network of national trainers, A&T supported training to implement these additional guidelines in five provinces, reaching about 65 hospitals and 600 health staff. These efforts closed the gap for EIBF between vaginal and C-section deliveries (see Figure 4).
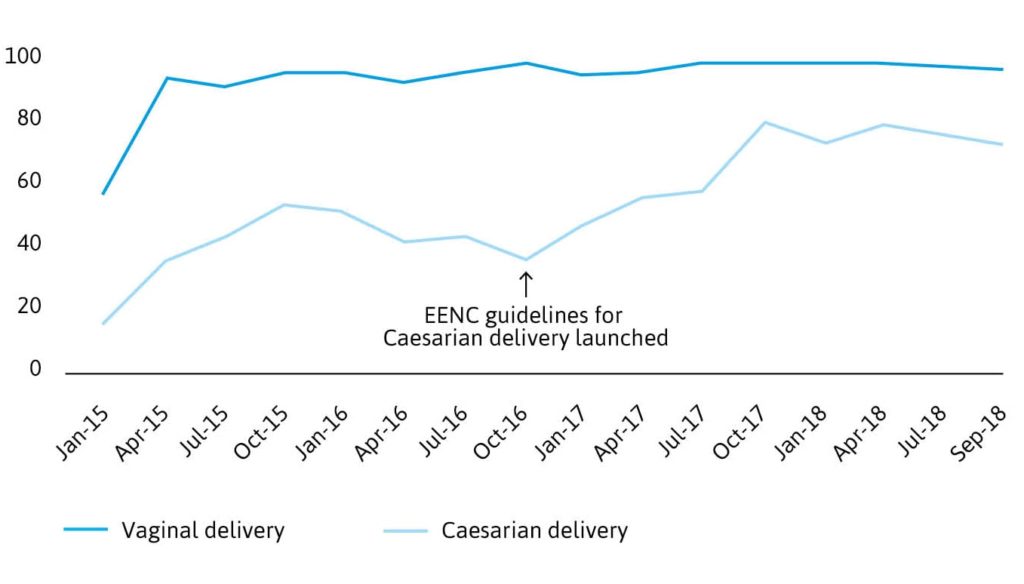
Figure 4: Percentage of newborns breastfed within one hour of birth
Success factors in increasing EIBF
Several factors enabled the widespread improvement in provider behaviour that supported the increase in EIBF and other EENC practices in Vietnam. Other institutions were simultaneously working to improve the enabling environment, for instance the WHO- and Unicef-led regional First Embrace initiative, which increased the demand for EENC. National-level interpersonal communication and mass media activities were also promoting EENC and EIBF. Based on the success in the seven provinces, A&T, with the Ministry and other organisations, helped to expand EENC, including support for EIBF to all major maternity hospitals in Vietnam.
At the facility level, the keys to success were as follows:
- Having explicit national-level EENC policies and facility guidelines for both vaginal and C-section deliveries increased provider adherence to key EENC procedures at
- Securing support from a dedicated group of breastfeeding champions in both the government and the facilities helped to get the policies implemented nationally. These champions, along with active leadership across facilities, held practitioners accountable to the new
- Providing on-site coaching and supportive supervision assured opportunities for regular feedback to continually strengthen health workers’ capacity and adherence.
- Ensuring regular monitoring data – a simple monitoring form that collected delivery and newborn care data from existing, required reports – allowed facility staff and the programme team to reward high-performing facilities, and redirect training and support resources to those institutions that were performing poorly. This information helped to facilitate timely decision making in target provinces, and it provided guidance for changes in policies and health provider-driven practices.
A&T continues to work with the Ministry of Health, Unicef, the WHO, and stakeholders in the region to improve breastfeeding. The experience and results from Vietnam have been disseminated to ten countries in the region through regional knowledge exchanges on breastfeeding-friendly health systems.
Representatives from other countries in the region have had the opportunity to observe best practices in breastfeeding support in health facilities in Vietnam, and to create their own country-specific workplans. A&T has also supported Danang to establish a regional learning and research centre for newborn care and human milk access to facilitate and sustain technical leadership, supervision and knowledge exchange for breastfeeding promotion and support.
Currently, a network of facilities is being established as Centres of Breastfeeding Excellence in Vietnam, Cambodia, Myanmar and Laos, to serve as models for promoting, protecting and supporting breastfeeding, and implementing EENC. These centres will be a hub of generating, sharing, and applying breastfeeding knowledge and policies in the region. Partners continue to work together to advocate for national laws and policies for better maternity protections and stronger regulations on the marketing of breast milk substitutes. Collectively, these efforts continue to contribute to the remarkable progress being made in policies and programmes that protect breastfeeding and give newborn babies the best start to life.
Acknowledgements
The author acknowledges the invaluable contributions of Roger Mathisen and the rest of the staff members at Alive & Thrive’s Association of Southeast Asian Nations (ASEAN) office who are involved in the implementation of this programming upon which the article is based. The Alive & Thrive initiative, managed by FHI 360, is currently funded by the Bill & Melinda Gates Foundation, the Government of Ireland, the Tanoto Foundation, and Unicef.
References can be found in the PDF version of the article.



